
Provider Access: WCRI Conference Observations

Last month’s post on provider access ended with a simple observation: expanding the pool of eligible providers only works if physicians want to swim in it.
At the recent WCRI conference, there was data and discussion on this topic that reaffirms that the pool itself is shrinking.
Hospital Closures Are Removing Options Nobody Has Replaced
WCRI presented research on the impact of hospital closures on injured worker access to care, and the numbers are worth sitting with. Nearly half of all hospital closures in recent years have occurred in rural areas. When a rural hospital closes, the average distance to the nearest emergency room increases by 5 miles … on top of baseline distances that already reach 15 miles in parts of the West.
In areas more than 20 miles from the nearest hospital, only 17% of injured workers access emergency care on the day of injury. In well-served areas, that number is 39%.
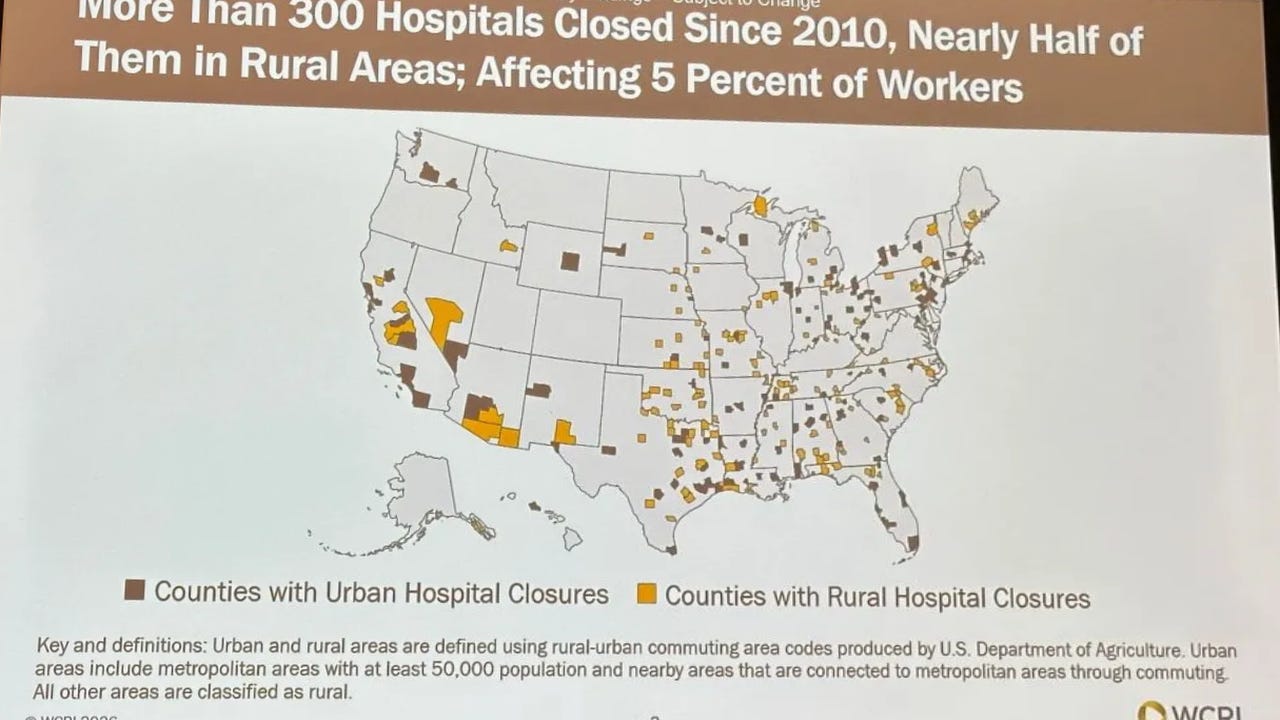
But here is the part that connects back to the friction argument. The aggregate cost data stayed relatively stable after closures. Workers adapted, they found urgent care centers and physician offices as alternatives.
What the data does not capture is the quality of those alternatives for workers’ comp specifically. An urgent care center that sees general patients is not the same as an occupational health clinic with workers’ comp billing experience, familiarity with state fee schedules, and willingness to navigate prior authorization. When a hospital closes and workers shift to alternative settings, they are often shifting to providers who have even less familiarity with workers’ comp … and even less patience for it.
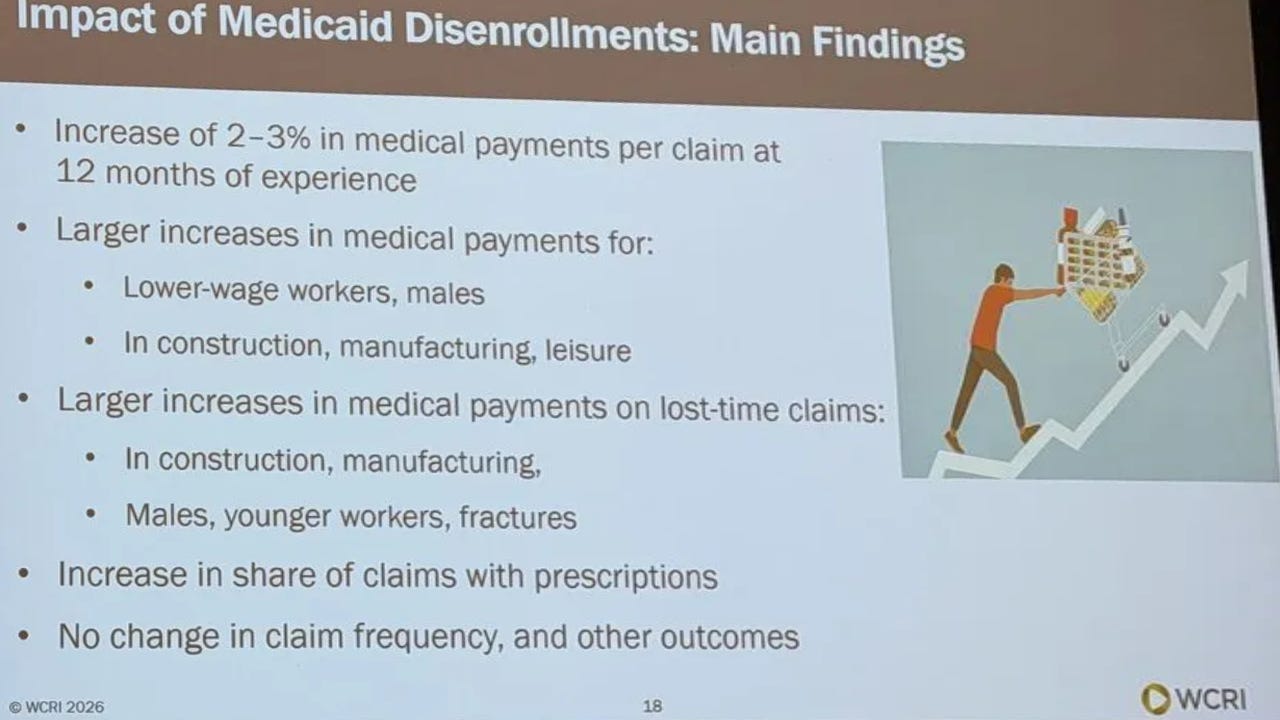
Medicaid Unwinding Is Changing Provider Behavior
The Medicaid unwinding research presented at WCRI pointed to another layer of the access problem that is easy to miss.
When workers lose Medicaid coverage, workers’ comp becomes a more prominent payer in their lives. Hospital payments in affected populations increased 6.7%. Non-hospital payments dropped 3.3%. The shift toward hospital-based care is partly a function of access … hospitals are required to treat, regardless of payer. Physician offices are not.
The same physicians who are already opting out of workers’ comp due to administrative burden now face a patient population that is more financially complicated than before. Workers who lost Medicaid may be carrying unresolved health conditions, may have deferred care, and may present with more complex comorbidities. For a physician already on the fence about workers’ comp participation, a more complicated patient with a more complicated payer is not a compelling reason to stay in the network.
Networks Help — But Not Where the Problem Is Worst
WCRI’s network effectiveness research confirmed what most in the industry already believe: networks work. The data showed a 27% reduction in overall claim costs … roughly $11,820 per claim, when accounting for reduced litigation, shorter disability duration, and lower benefit delivery expenses.
But the study also confirmed that network effects are significantly smaller in rural areas. Rural medical payment savings run at 20% versus 28% in urban markets. Many rural network effects do not reach statistical significance at all.
This is the geographic version of the friction problem. The physicians willing to participate in workers’ comp networks are concentrated in urban and suburban markets where work comp volume justifies the administrative investment. In rural areas, where a physician might see one or two workers’ comp patients a month (or year), the math does not work the same way. The network exists on paper. In practice, the injured worker is navigating the same gaps.
The Access Problem Has Layers
Hospital closures are removing providers and replacing them with alternatives that may be less equipped for workers’ comp. Medicaid disenrollment is likely creating a more complex patient population that further strains physician willingness to participate. Network tools that generate real savings in cities are less effective in the markets where access is most fragile.
None of this is a reason for fatalism. The employers on WCRI’s access to care panel presented several solutions they have implemented to address this problem; direct contracting, telemedicine, on-site clinics, and transportation assistance. Texas regulators hosted 24 live webinars last year to educate providers and reduce friction from the regulatory side. These are workable solutions.
But they require someone deciding that the physician and injured worker experience inside the workers’ comp system is worth investing in … not just expanding who is eligible to participate.
To repeat the conclusion of the prior post
The underlying problem remains: workers’ compensation is more difficult, more burdensome, and less integrated than commercial health. Until that changes, through better technology, streamlined authorization, and improved payment processes, physicians will continue to opt out and injured workers will feel it.
Expanding the pool only works if physicians want to swim in it.
Hospital closures, medicaid disenrollment, and other factors will continue to put pressure on provider access. Workers’ comp stakeholders will need to continue focusing on this challenge to avoid bad outcomes, clinically and financially.
Excellent summary of the topics at WCRI Ben - thanks for sharing.